RadFlow AI — KI-gestützter Radiologie-Workflow-Assistent
Verkürzung der CT-Befundungszeit um 38 % durch nahtlose KI-Integration und leistungsstarkes DICOM-Rendering*


Ein führendes Netzwerk für diagnostische Bildgebung mit 12 radiologischen Zentren in drei Bundesstaaten stand vor einem kritischen Wendepunkt: Das Scan-Volumen wuchs jährlich um 22 %, während die Anzahl der Radiologen stagnierte. Die Folge waren zunehmende Überlastung, steigende Bearbeitungszeiten (TAT, die vertragliche SLAs um 15 % überschritten) und eine messbare Verschlechterung der Erkennungsgenauigkeit bei Spätschichtbefundungen.
Codebridge wurde beauftragt, einen HIPAA-konformen, Cloud-nativen, KI-gestützten Diagnose-Arbeitsbereich zu entwickeln, der in bestehende PACS integriert ist und Computer Vision direkt in den klinischen Workflow integriert, ohne die bestehende PACS-Infrastruktur zu stören oder Radiologen zum Erlernen neuer Tools zu zwingen. Der Auftrag war klar: menschliche Expertise zu erweitern, niemals zu ersetzen.
Im Rahmen eines 24-wöchigen Projekts lieferte ein achtköpfiges Codebridge-Team eine produktionsreife „Human-in-the-Loop“-Plattform, die die durchschnittliche CT-Befundungszeit von 15,2 auf 9,4 Minuten reduzierte (ein Effizienzgewinn von 38 %), eine 96%ige Sensitivität bei der Erkennung von Knoten unter 4 mm beibehielt und eine Bildwiedergabe in unter einer Sekunde erreichte, selbst über Satellitenverbindungen mit geringer Bandbreite, die von den ländlichen Teleradiologie-Standorten des Kunden genutzt werden.
Die Lösung bestand eine unabhängige klinische Validierungsstudie (n=2.400 Scans, doppelblinde Ausführung), ist im Einklang mit den FDA-Regulierungsrichtlinien für Software als Medizinprodukt (SaMD) der Klasse II konzipiert und ist seit über 9 Monaten ohne gemeldete kritische Systemausfälle in Betrieb.
Kundenprofil & Strategischer Kontext
Der Kunde ist ein privat geführtes Netzwerk für diagnostische Bildgebung mit einem jährlichen Umsatz im dreistelligen Millionenbereich. Es fungiert als vertraglicher Radiologieanbieter für mehrere Krankenhaussysteme und ein großes Netzwerk ambulanter Bildgebungszentren in mehreren Bundesstaaten. Ihr Betrieb verarbeitet wöchentlich über 500 Thorax-CT-Scans, wobei saisonale Spitzenwerte in Zeiten erhöhter Atemwegserkrankungen 700 Scans überschreiten.
Wettbewerbsdruck & Marktdynamik
Der Markt für diagnostische Bildgebung befindet sich in einem strukturellen Wandel. Die Erwartungen der überweisenden Ärzte an die Bearbeitungszeit haben sich von 48 Stunden auf die Befundung am selben Tag für Routineuntersuchungen verkürzt. Gleichzeitig zeigen nationale Arbeitsmarktanalysen einen wachsenden Radiologenmangel auf, der durch steigende Bildgebungs-Volumina und den Ärzteschwund verursacht wird. Für den Kunden war eine bloße Personalaufstockung keine nachhaltige Lösung – sie benötigten einen skalierbaren Technologie-Multiplikator.
Strategische Ziele
Der Kunde definierte vier nicht verhandelbare Erfolgskriterien:
- Die durchschnittliche CT-Befundungszeit um mindestens 25 % reduzieren, ohne die diagnostische Sensitivität zu beeinträchtigen.
- Eine nahtlose Integration in die bestehenden Enterprise-PACS und strukturierten Befundungssysteme aufrechterhalten.
- Die Lösung gemäß den Entwicklungsstandards IEC 62304 und ISO 13485 konzipieren, um einen zukünftigen FDA 510(k)-Zulassungsweg zu unterstützen.
- Die vollständigen Rechte am geistigen Eigentum an allen trainierten Modellen und gesammelten Datensätzen behalten.
Die Herausforderung: Ein mehrdimensionales Einschränkungssystem
In einer fokussierten Analysephase arbeitete unser Team für klinische Technik mit Radiologen an mehreren Standorten zusammen, um die betrieblichen, technischen und regulatorischen Reibungspunkte in deren CT-Arbeitsablauf zu verstehen. Was sich zeigte, war kein einzelner Engpass, sondern ein vielschichtiges Systemproblem – eines, das nicht durch den Einsatz eines weiteren eigenständigen KI-Algorithmus gelöst werden konnte.
Workflow Fragmentation & Cognitive Load
Radiologists were required to operate across multiple disconnected systems simultaneously: the primary PACS viewer for image interpretation, a separate AI interface accessed outside the core viewer, and a voice-dictation reporting system.
This fragmented environment introduced consistent context-switching overhead — often adding several minutes per study — while forcing clinicians to manually reconcile AI findings with the primary imaging interface.
Time-motion analysis revealed that roughly one-third of total reading time was consumed by non-interpretive tasks: navigating between systems, re-orienting spatial context after window switches, manually transferring measurements into structured reports, and verifying external AI annotations.
The cost was not only temporal but cognitive. Research in interruption science shows that even brief context shifts degrade diagnostic attention. In high-volume environments, this compounding cognitive load contributes directly to fatigue, variability in interpretation, and burnout.
As one clinical leader summarized during discovery:
“We didn’t need another black-box algorithm. We needed a workspace that supports how radiologists actually think and work.”
Data Gravity & Rendering Latency
High-resolution chest CT studies routinely generate hundreds of DICOM instances per case, with full datasets often exceeding several hundred megabytes.
The client’s legacy remote access infrastructure introduced significant latency during peak usage periods. Initial study load times frequently exceeded acceptable thresholds, and scroll-through performance degraded under network congestion — particularly for rural teleradiology sites operating on low-bandwidth satellite connections.
During seasonal respiratory peaks, these constraints translated into growing backlogs, delayed turnaround times, and increased reliance on after-hours coverage.
This was not simply a network problem; it was an architectural one. Any AI overlay had to process large volumetric datasets while preserving sub-second interaction inside the radiologist’s primary workspace.
False Positives & Trust Erosion
The client had previously piloted multiple commercial AI solutions. While technically functional, these tools generated elevated false-positive volumes, particularly in cases involving post-surgical changes, granulomatous disease, and motion artifacts.
Each false positive required manual verification and documentation — effectively adding work rather than removing it.
More concerning was the downstream effect on clinician behavior. Over time, a majority of radiologists reported developing the habit of dismissing AI findings without review. In such scenarios, AI ceases to function as a productivity enhancer and instead becomes a liability exposure layer.
An AI system that is routinely ignored delivers negative operational value.
Regulatory & Compliance Envelope
Beyond workflow and performance constraints, the solution needed to operate within a strict regulatory framework.
This included:
- HIPAA and HITECH requirements for protected health information
- Alignment with IEC 62304 software lifecycle processes
- Development traceability compatible with a future FDA 510(k) pathway
- Full audit logging of model updates and deployment changes
- State-level teleradiology data handling restrictions
The mandate was clear: any performance gains must be achieved without compromising compliance posture or introducing regulatory exposure.
Umfang der Arbeit
Klinische Analyse & Architekturdefinition (Wochen 1-3)
Integrierte Analyse klinischer Arbeitsabläufe, Infrastruktur-Audit, Bewertung regulatorischer Lücken und formale Architekturdefinition, abgestimmt auf zukünftige FDA-Einreichungswege.
Plattformgrundlage & Sichere Infrastruktur (Wochen 4-8)
Entwicklung des diagnostischen Kern-Viewers mit DICOMweb-Integration, sicherem SSO (SAML), Bereitstellung von Cloud-Infrastruktur und IEC 62304-konformen Entwicklungsprozessen.
KI-Modellintegration & Workflow-Einbettung (Wochen 9–14)
Modelltraining und -optimierung auf großen CT-Datensätzen, Bereitstellung über Hochleistungs-Inferenz-Pipelines, Reduzierung von falsch positiven Ergebnissen und nahtlose Einbettung in den primären Arbeitsablauf des Radiologen.
Klinische Pilotphase & Leistungsoptimierung (Wochen 15–18)
Kontrollierte standortübergreifende Bereitstellung mit Feedbackschleifen aus der Praxis, UX-Optimierungen, Integration intelligenter Triage und Shadow-Mode-Validierung zur Leistungsbewertung im Vergleich zum bestehenden Arbeitsablauf.
Unabhängige Validierung & Unternehmensweite Einführung (Wochen 19–24)
Unabhängige klinische Validierungsstudie, Last- und Sicherheitstests, gestaffelte Bereitstellung an 12 Standorten, Schulung des Klinikpersonals und Vorbereitung der Dokumentation für die Abstimmung vor der FDA 510(k)-Einreichung.
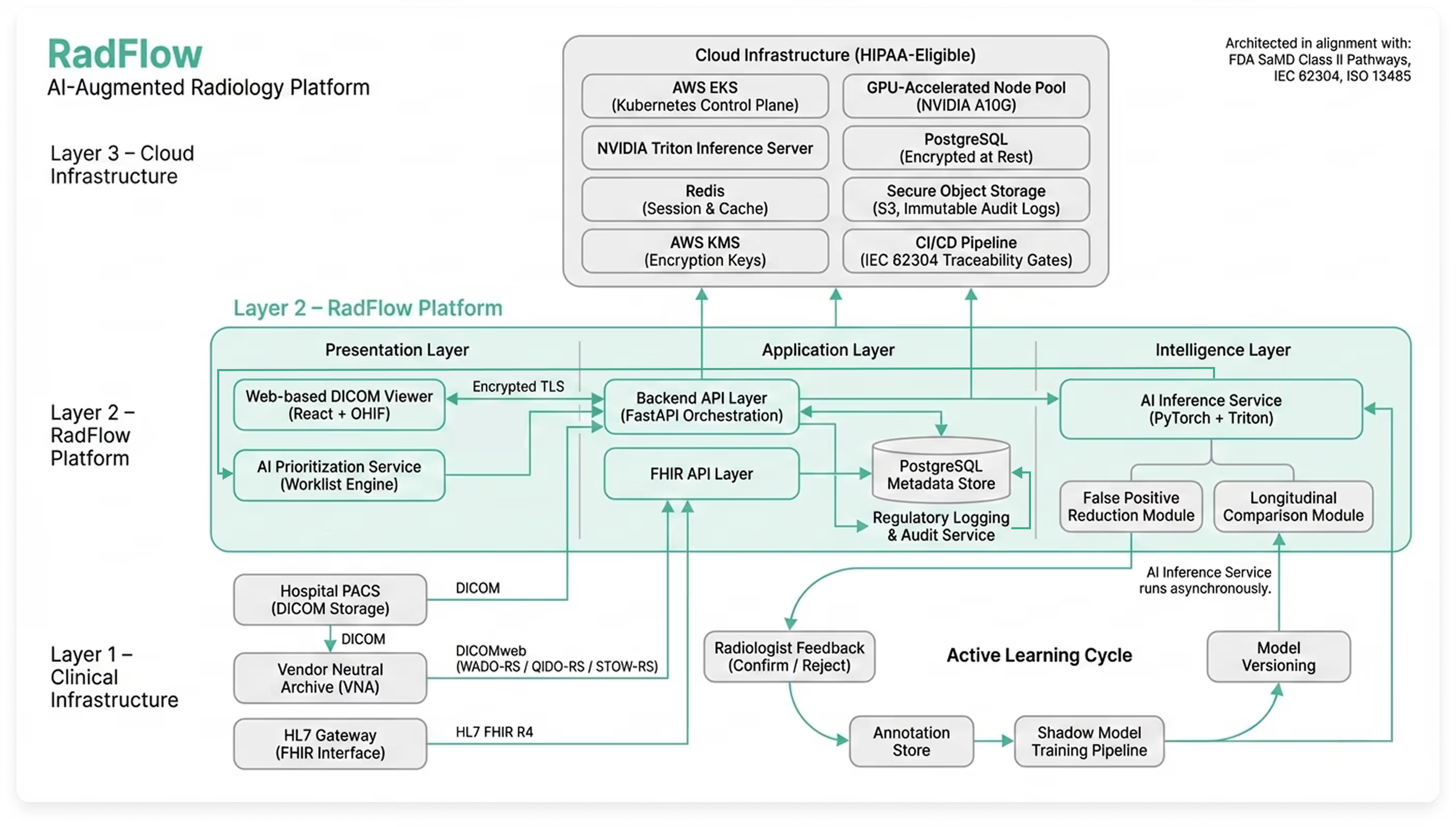
Lösungsarchitektur: KI-gestützter diagnostischer Arbeitsbereich
Anstatt ein eigenständiges KI-Modell zu entwickeln, das von der klinischen Realität losgelöst ist, entwickelte Codebridge einen Cloud-nativen, KI-gestützten diagnostischen Arbeitsbereich, der darauf ausgelegt ist, parallel zur bestehenden PACS-Infrastruktur zu funktionieren und gleichzeitig Triage-, Erklärbarkeits- und Governance-Funktionen einzuführen.
Die Plattform fungiert als unabhängige webbasierte Bildgebungsumgebung, vollständig synchronisiert mit dem Vendor Neutral Archive (VNA) und den Berichtssystemen des Kunden. Radiologen nutzen weiterhin ihre bestehende PACS-Arbeitsliste, können aber jede Studie mit einem Klick über eine sichere SAML-Authentifizierung im KI-Arbeitsbereich öffnen.
Das Ergebnis ist kein Algorithmus – sondern eine vollständige Diagnoseschicht, die Interpretation, Priorisierung und Überwachung verbessert, ohne etablierte Arbeitsabläufe zu stören.
Vereinheitlichter diagnostischer Arbeitsbereich
Die Plattform besteht aus fünf integrierten Modulen, die direkt in der Produktions-Benutzeroberfläche (UI) widergespiegelt werden:
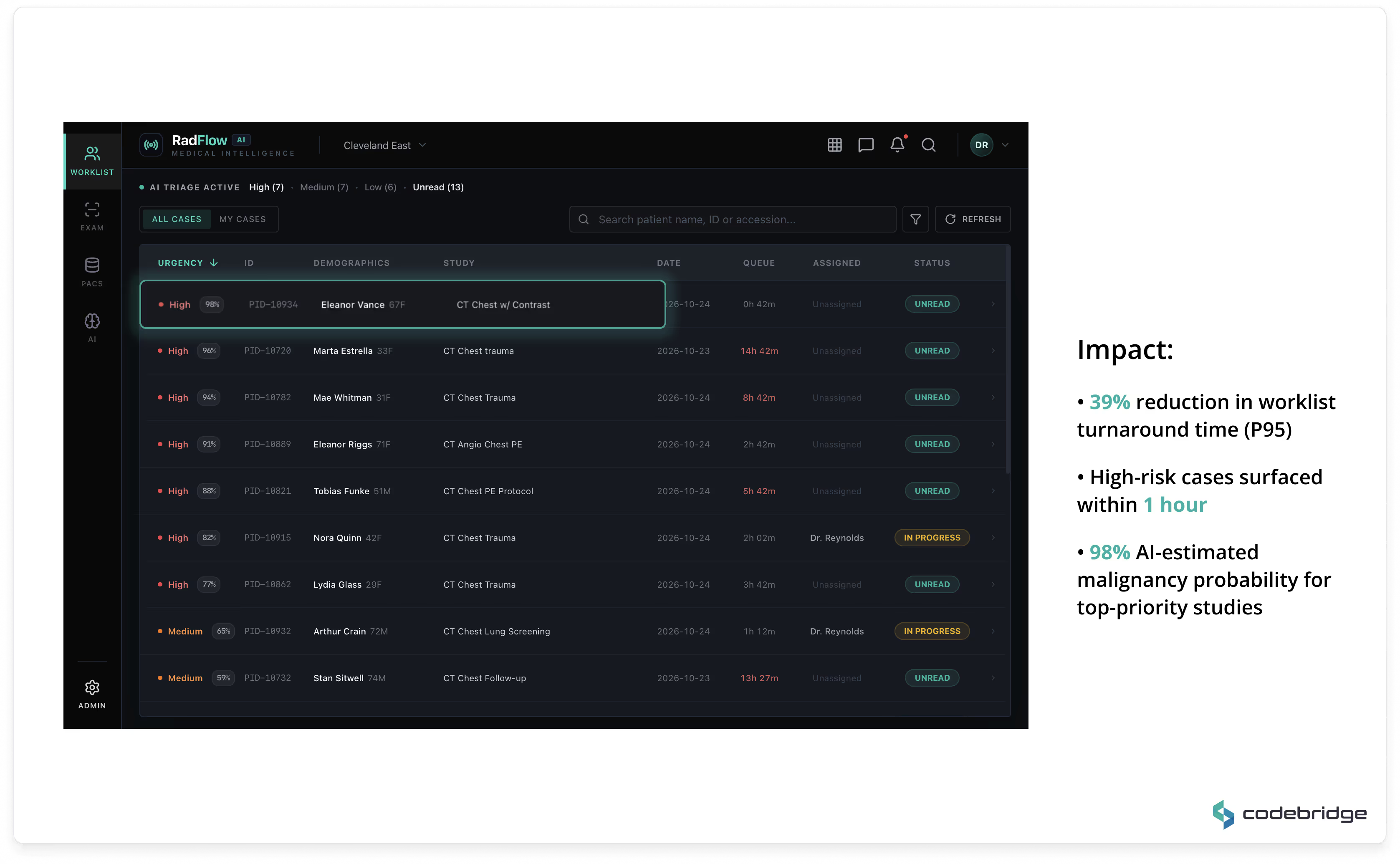
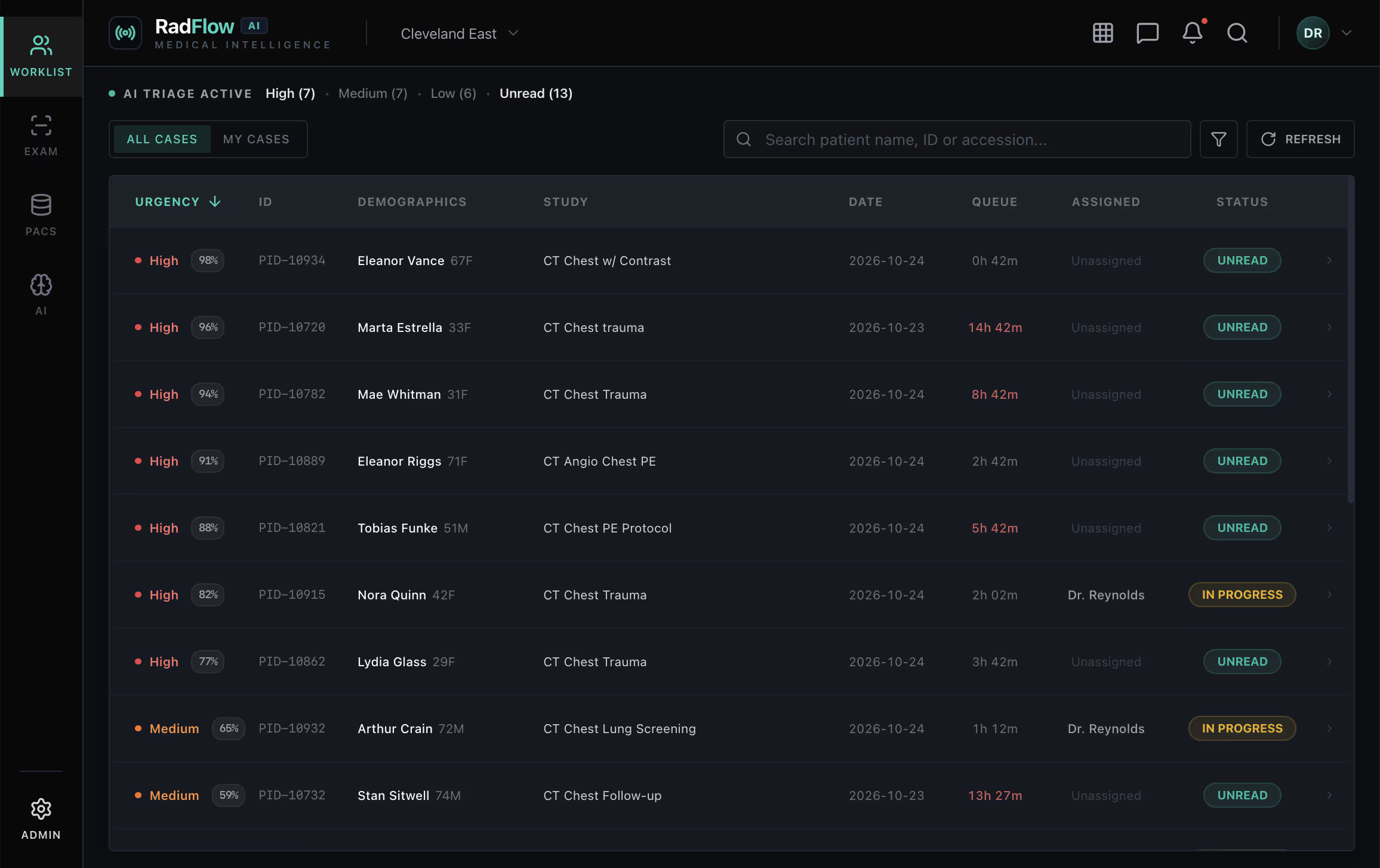
Arbeitsliste & KI-Triage
Eine Echtzeit-Prioritätenarbeitsliste ordnet Studien nach KI-geschätzter Malignitätswahrscheinlichkeit und Dringlichkeitsbewertung. Fälle mit hohem Risiko werden automatisch hochgestuft, was eine frühere Überprüfung bei hohem Scan-Aufkommen ermöglicht.
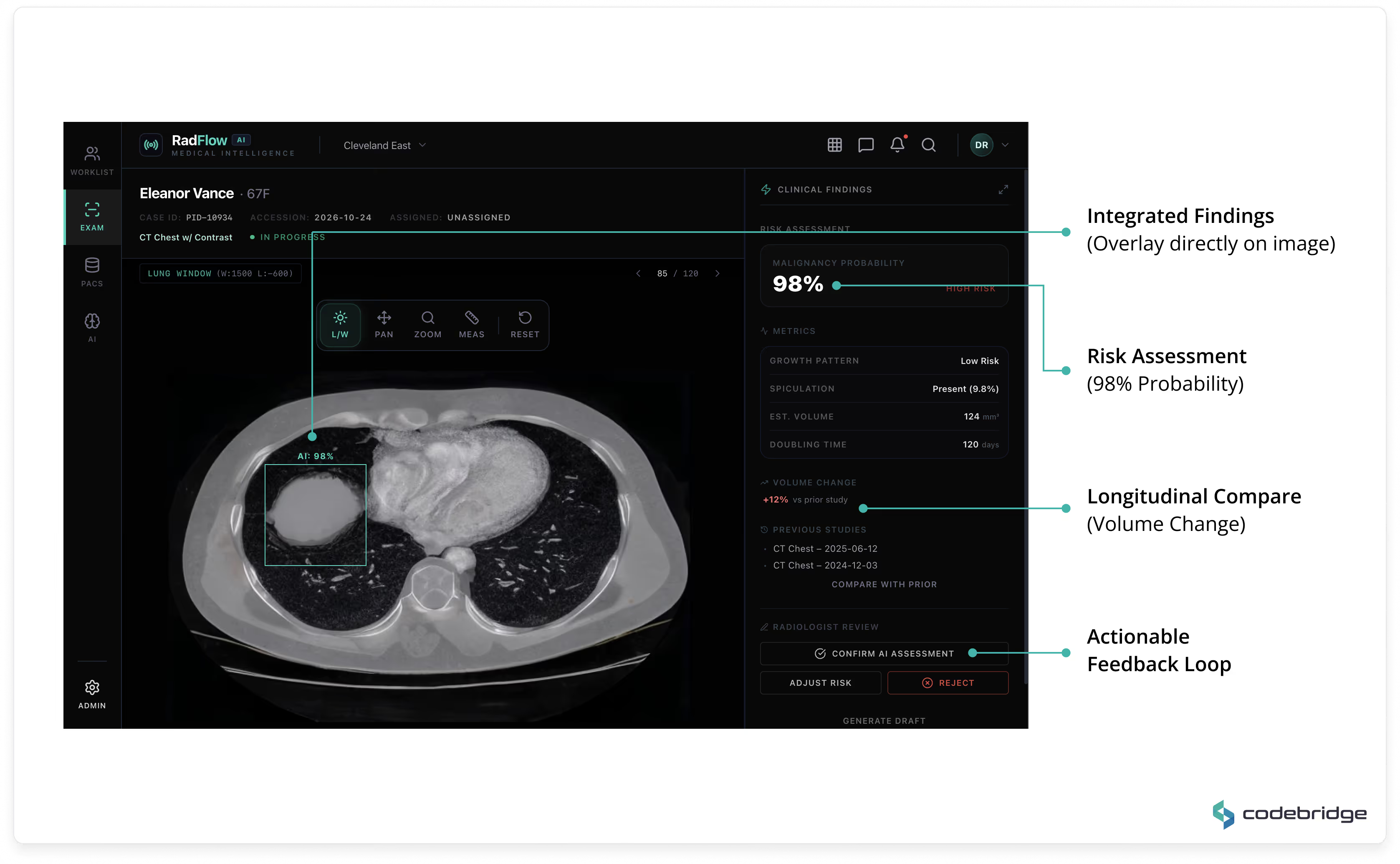
KI-erweiterter Viewer
Ein GPU-beschleunigter Web-Viewer (basierend auf OHIF und Cornerstone.js) unterstützt axiale, MPR- und volumetrische Darstellung direkt im Browser. KI-Erkennungen werden als strukturierte Overlays angezeigt mit:
- Malignitätswahrscheinlichkeit
- volumetrische Messungen
- Verdopplungszeit
- morphologische Deskriptoren
- Vergleich mit Vorstudien
Alle KI-Befunde können ein- und ausgeblendet werden und stehen vollständig unter der Kontrolle des Radiologen.
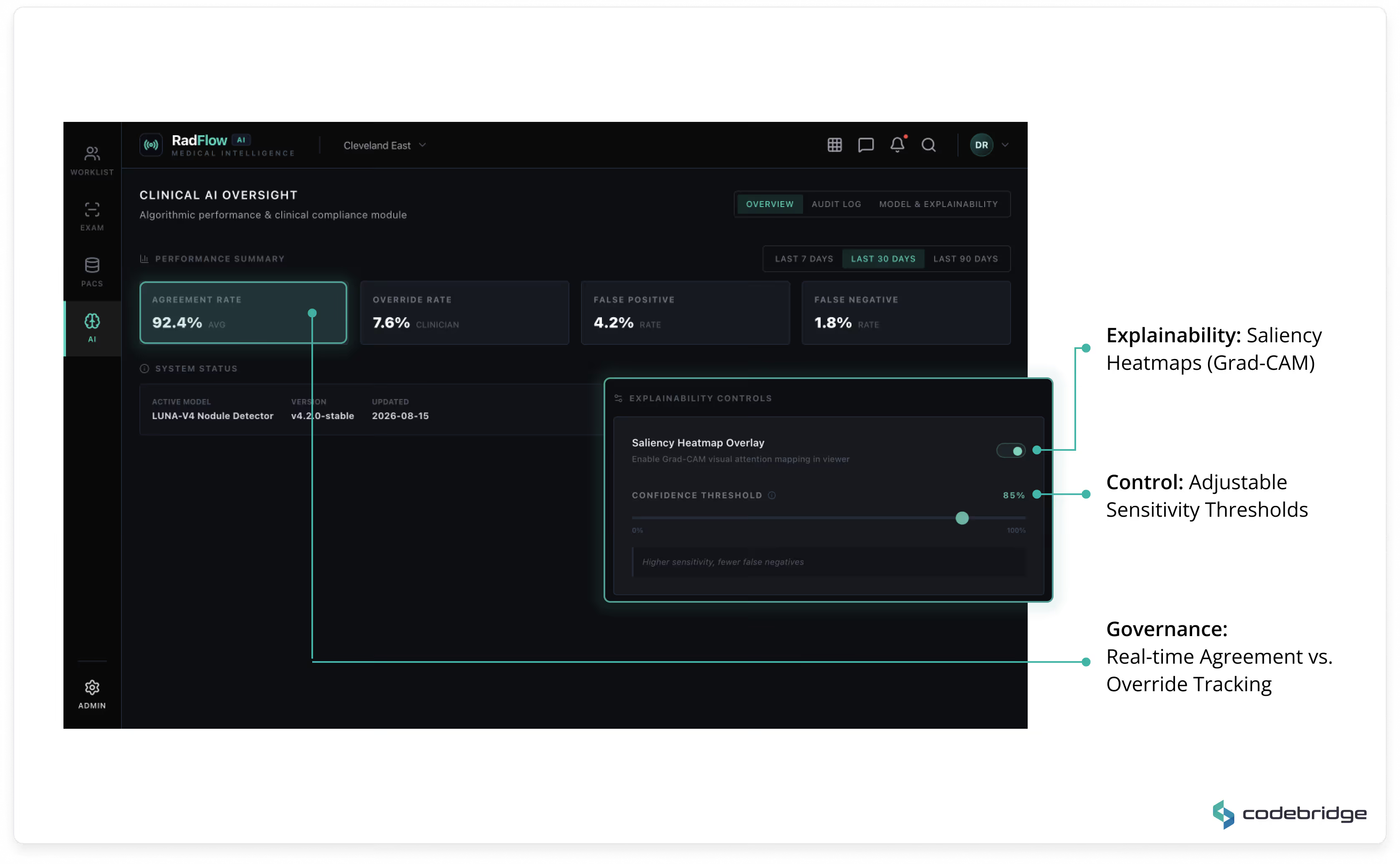
Klinisches KI-Überwachungsmodul
Ein Governance-Dashboard erfasst:
- Übereinstimmungsrate
- Übersteuerungsrate
- Metriken für falsch positive / falsch negative Ergebnisse
- Modellversionshistorie
- Erklärbarkeitskontrollen (Grad-CAM-Saliency-Maps)
- Konfiguration der Konfidenzschwelle
Dieses Modul gewährleistet eine transparente Leistungsüberwachung und regulatorische Nachvollziehbarkeit.
Audit- und Erklärbarkeits-Protokolle
Jede KI-gestützte Entscheidung wird protokolliert mit:
- Modellversion
- Zeitstempel
- Status der klinischen Übersteuerung
- Ablehnungsgrund (falls zutreffend)
Alle Änderungen werden in einem unveränderlichen Audit-Speicher gespeichert, der den regulatorischen Erwartungen entspricht.
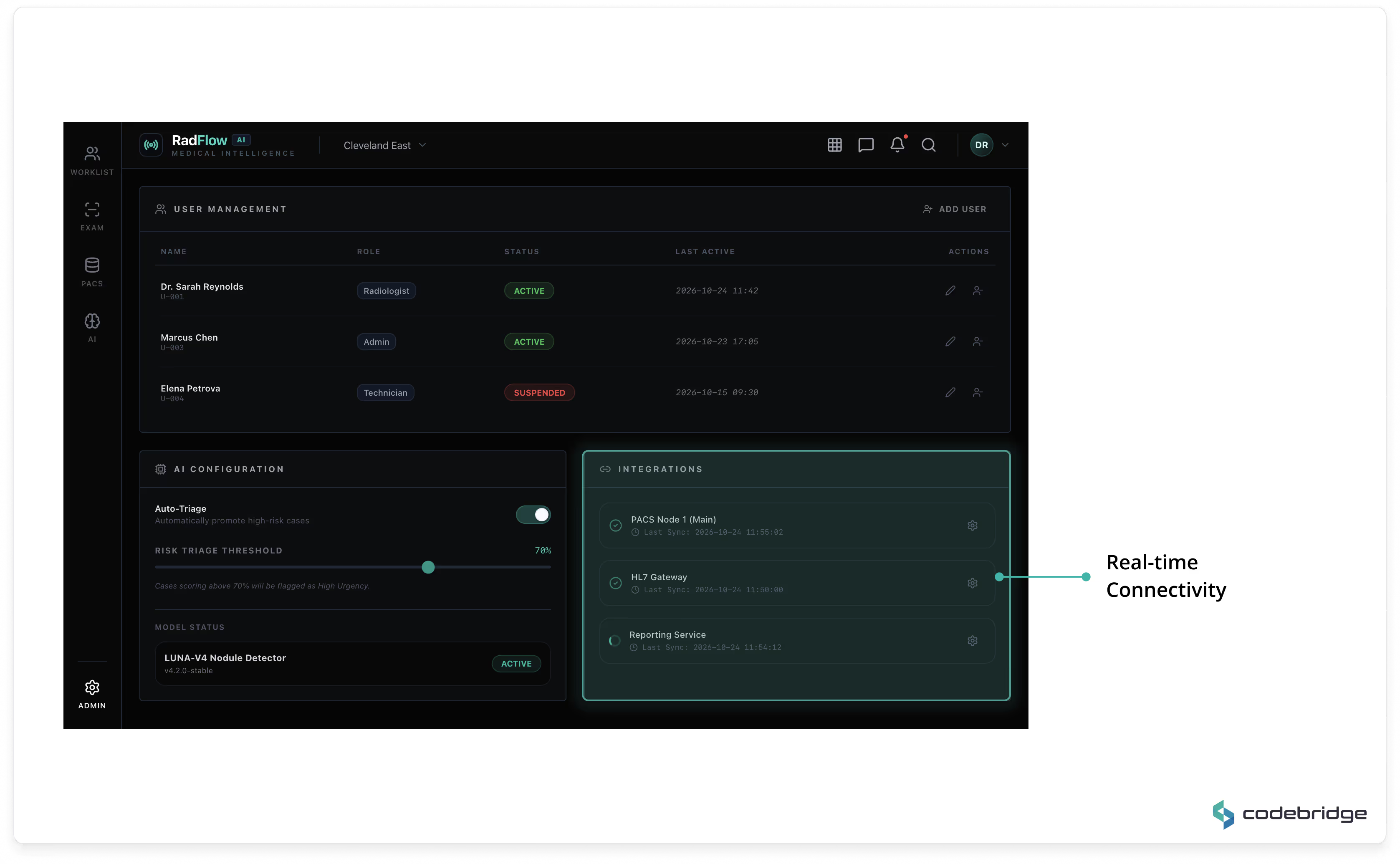
Administrations- und Integrationsschicht
Umfasst Benutzerverwaltung, rollenbasierte Zugriffskontrolle (RBAC), KI-Konfigurationseinstellungen und Überwachung der PACS/VNA-Integration.
Hochleistungs-Web-Bildgebungs-Engine
Der Viewer ist vollständig browserbasiert und erfordert keine lokale Installation.
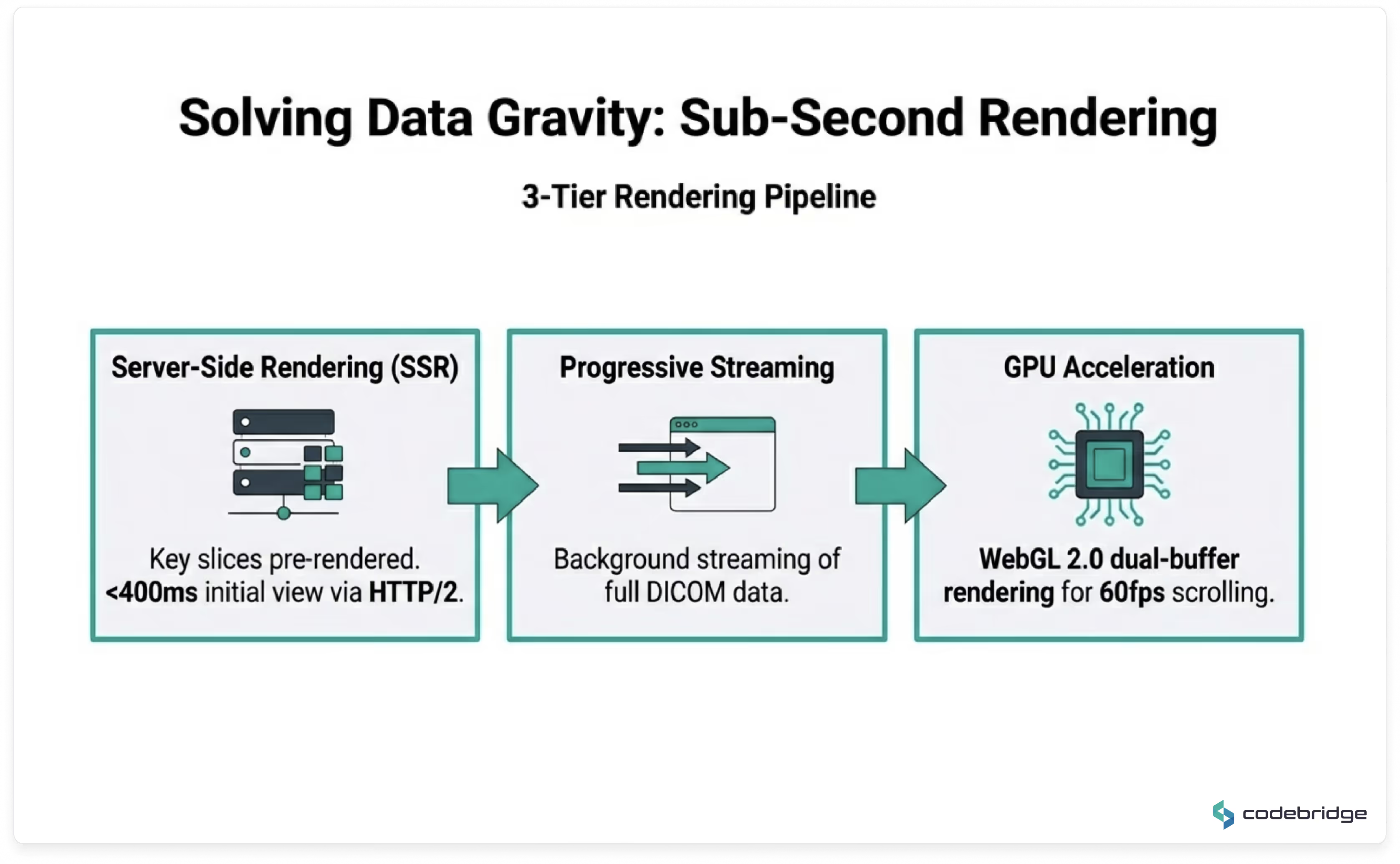
Hauptmerkmale:
- Progressives DICOM-Streaming über DICOMweb (WADO-RS / QIDO-RS / STOW-RS)
- GPU-beschleunigtes Rendering mit WebGL 2.0
- Adaptive Bandbreitenkomprimierung für ländliche Satellitenstandorte
- Lokales Browser-Caching für kürzlich geöffnete Studien
- DICOM-Parsing im Hintergrund über WebWorkers
Durchschnittliche Zeit bis zur ersten Darstellung: < 400 ms in optimierten Netzwerken.
Navigation in unter einer Sekunde, sobald der vollständige Datensatz geladen ist.
Das System unterstützt dünnschichtige Thorax-CT-Studien (300–500 MB) ohne wahrnehmbare Blockierung der Benutzeroberfläche.
KI-Inferenz & Modell-Lebenszyklus
Die KI-Inferenz läuft asynchron bei der Aufnahme der Studie in das VNA ab.
Wenn ein Radiologe einen Fall öffnet, ist die KI-Analyse bereits verfügbar.
Modell-Design
- 3D Feature Pyramid Network (FPN)
- ResNet-50 Encoder-Backbone
- Optimiert für die Erkennung kleiner Läsionen (Noduli unter 4 mm)
- Netzwerk zur Reduzierung falsch-positiver Ergebnisse
- Longitudinales Vergleichsmodul zum Abgleich mit früheren Studien
Die anfängliche Falsch-Positiv-Rate wurde von 4,1 auf 0,8 pro Scan reduziert.
Nach 9 Monaten aktiven Lernens: weiter auf 0,4 reduziert.
Der Sensitivitäts-Benchmark wird bei 96 % gehalten.
Infrastruktur und Skalierbarkeit
Das System wird in einer HIPAA-konformen Cloud-Umgebung bereitgestellt.
Kernkomponenten:
- FastAPI-Backend
- PostgreSQL (klinische Metadaten)
- Redis (Caching/Sitzungsstatus)
- RabbitMQ (asynchrone Orchestrierung)
- NVIDIA Triton Inference Server auf AWS EKS
- GPU-Knoten mit Auto-Scaling-Richtlinien
Durchschnittliche End-to-End-Inferenzlatenz: ca. 47 Sekunden pro CT-Untersuchung.
Auto-Scaling gewährleistet eine kosteneffiziente GPU-Bereitstellung während saisonaler Spitzenlast.
Regulatorische und Compliance-Ausrichtung
Die Plattform wurde in Übereinstimmung mit den regulatorischen Pfaden der FDA für Software als Medizinprodukt (SaMD) der Klasse II konzipiert.
Der Entwicklungslebenszyklus umfasst:
- Rückverfolgbarkeit gemäß IEC 62304 in CI/CD
- ISO 13485-konformes Änderungsmanagement
- Umfassende Audit-Protokollierung
- Modellversionsverfolgung
- Hashing von Trainingsdatensätzen
- Unveränderliche Bereitstellungsprotokolle
Die Benutzeroberfläche enthält sichtbare Platzhalter für den FDA-Zulassungsstatus, um die Bereitschaft für die regulatorische Kennzeichnung nach der Validierung sicherzustellen.
Technologie-Stack
Jede Technologieentscheidung basierte auf drei Kriterien: klinische Zuverlässigkeit, regulatorische Rückverfolgbarkeit und langfristige Wartbarkeit ohne Anbieterbindung.
Teamzusammensetzung
Codebridge setzte ein funktionsübergreifendes Team von 8 Ingenieuren mit umfassendem Fachwissen in der medizinischen Bildgebung, regulatorischer Compliance und Hochleistungs-Webanwendungen ein.
Technologien, die wir in diesem Projekt verwenden
Schlüsselergebnisse & Klinische Auswirkungen
Alle unten aufgeführten Metriken wurden durch eine formelle 60-tägige Leistungsüberprüfung nach der Bereitstellung, durchgeführt vom Clinical AI Governance Board des Kunden, validiert und durch Ergebnisse einer unabhängigen doppelblinden klinischen Validierungsstudie ergänzt.
Reduction in Average CT Reading Time
From 15.2 minutes to 9.4 minutes per study, validated across 4,800+ CT cases.
Sub-4mm Nodule Detection Sensitivity
Validated in a double-blind study (n=2,400), exceeding the predefined 93% acceptance threshold.
False Positives per Scan
Reduced from 4.1 (previous vendor solution) to 0.4 through a dedicated false-positive reduction network and 9 months of active learning.
Progressive Rendering Time
70% improvement over legacy VPN-based viewers; fully functional over satellite connections (12 Mbps).
Estimated Annual Operational Impact
Productivity gains equivalent to approximately 3 FTE radiologists, plus a significant reduction in after-hours coverage costs at rural sites.
Detaillierter Leistungsvergleich
Einfluss auf den klinischen Workflow
Die Smart Triage-Funktion ordnet Studien automatisch nach der KI-geschätzten Malignitätswahrscheinlichkeit, wodurch Radiologen Hochrisikofälle während Spitzenzeiten des Bildgebungsaufkommens priorisieren können.
Innerhalb der ersten sechs Monate wurden 23 Fälle mit hoher Malignitätswahrscheinlichkeit innerhalb einer Stunde nach der Akquisition überprüft (im Vergleich zu einem früheren Durchschnitt von 4,5 Stunden). Laut dem Chief Medical Officer des Kunden trug der beschleunigte Triage-Pfad während des Evaluierungszeitraums zu Früherkennungen bei.
Vertrauenswiederherstellung
Das bedeutendste qualitative Ergebnis war die Wiederherstellung des Vertrauens der Radiologen in die KI-Unterstützung.
Der Radiologen-Vertrauens-Score – eine interne Umfragestatistik, die den Prozentsatz der Radiologen misst, die routinemäßig KI-Befunde überprüfen – stieg von 27 % zu Beginn auf 89 % nach sechs Monaten.
Diese Veränderung wurde nicht durch politische Vorgaben oder Schulungsinitiativen erreicht, sondern durch technische Disziplin:
• 90 % Reduzierung falsch-positiver Befunde
• Nahtlose Integration im Viewport
• Volle Erklärbarkeit und Kontrolle durch den Kliniker
„Zum ersten Mal macht mich die KI tatsächlich schneller statt langsamer. Ich habe aufgehört, sie zu ignorieren, etwa in der zweiten Woche des Pilotprojekts.“ — Leitender Radiologe, Standort 3
Strategischer Wert & Wert des geistigen Eigentums
Gemäß den Vertragsbedingungen behält der Kunde das vollständige Eigentum am geistigen Eigentum (IP) an:
- Neu trainierte Modellgewichte
- Über 4.200 von Experten beurteilte Annotationen
- Der vollständige Code der KI-erweiterten Plattform
Der Vorstand des Kunden hat diesen Vermögenswert als strategisches Unterscheidungsmerkmal bei bevorstehenden Vertragsverlängerungen mit Krankenhäusern und als grundlegenden Bestandteil ihres geplanten FDA-Zulassungswegs identifiziert.
Zukünftige Pläne
Die Plattform wurde als skalierbare Grundlage für die Erweiterung KI-gestützter Radiologiefunktionen über verschiedene Modalitäten und klinische Bereiche hinweg konzipiert. Der Kunde und Codebridge haben sich auf eine strategische Phasen-Roadmap für die weitere Entwicklung geeinigt.
Phase 2 — Aktive Entwicklung
- Erweiterung der KI-Triage-Funktionen auf Thorax-Röntgenuntersuchungen
- Integration der automatisierten Lung-RADS-Bewertung
- Nachverfolgung von Folgemaßnahmen im geschlossenen Kreislauf über die Epic EHR-Integration
Phase 3 — Strategische Erweiterung
- Unterstützung für Abdomen-CT (Erkennung von Leberläsionen, Charakterisierung von Nierensteinen)
- Studienübergreifende Längsschnitt-Dashboards für die Onkologie-Überwachung
- Generierung von Berichten in natürlicher Sprache zur Unterstützung strukturierter Berichterstattungsworkflows
Regulierungspfad
Die gesammelte IEC 62304-Dokumentation, unabhängige klinische Validierungsdaten und die Design-History-Datei für die Regulierung belegen die Bereitschaft für einen FDA 510(k) Pre-Submission-Weg. Eine Pre-Submission-Einreichung ist für das 2. Quartal 2026 geplant, vorbehaltlich der Prüfzeiten der Aufsichtsbehörden.
*Hinweis: Aufgrund von NDA-Beschränkungen wurden der Kundenname und spezifische institutionelle Kennungen anonymisiert. Alle Leistungsmetriken und Validierungsergebnisse basieren auf realen Produktionsdaten.
FAQ-Bereich (Technischer Einblick)
How did you achieve native PACS-level performance in a browser-based CT viewer?
High-resolution chest CT studies may contain 600+ thin-slice images. Diagnostic cine-mode scrolling requires rendering 30–60 frames per second without perceptible latency — a threshold traditionally achievable only on native PACS workstations.
To meet this requirement in a zero-install browser environment, we implemented a dual-buffer WebGL rendering architecture. While the current frame is displayed from one GPU texture buffer, subsequent frames are decoded in parallel using WebWorkers and preloaded into a secondary GPU buffer. On scroll, buffers swap instantly.
This approach enables sustained 60fps cine-mode performance, even for 300–500MB CT datasets, delivering workstation-grade responsiveness within a secure web environment.
How was the false-positive rate reduced from 4.1 to 0.4 per scan?
False positives were the primary barrier to clinical adoption in prior AI pilots. Rather than relying solely on generic model tuning, we engineered a dedicated false-positive reduction pipeline.
In regions with elevated prevalence of benign granulomatous disease, calcified nodules represented a dominant source of misclassification. We developed a post-processing classifier trained on a curated dataset of confirmed benign cases from the client’s anonymized archive. This classifier operates as a secondary filter layered atop the primary detection network.
The result was a 90% reduction in false positives while preserving 96% sensitivity for sub-4mm nodules — restoring clinician trust without sacrificing diagnostic rigor.
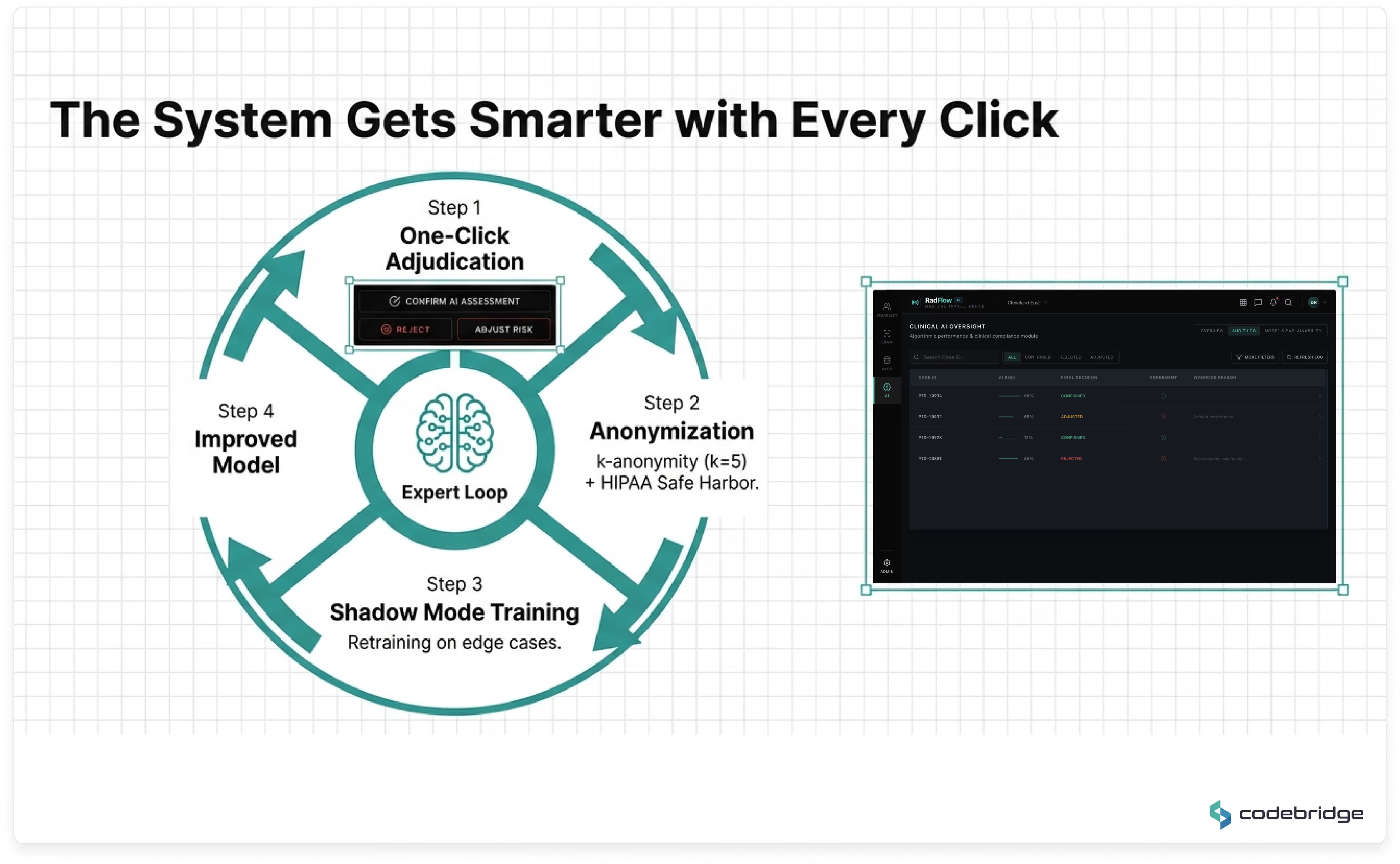
How does the platform support HIPAA-compliant active learning?
Continuous model improvement requires careful separation of clinical operations and research-grade data processing.
We implemented a multi-layer compliance architecture:
- DICOM de-identification aligned with the HIPAA Safe Harbor method (removal of 18 identifier categories)
- k-anonymization (k=5) for structured demographic attributes
- Segregated encrypted data lake for annotations
- Isolated VPC environment for retraining pipelines
- No public internet egress from model training infrastructure
An independent third-party compliance audit validated that the architecture satisfies HIPAA and internal governance requirements while enabling structured active learning.
Why build a full diagnostic workspace instead of integrating a standalone AI plugin?
Previous AI pilots demonstrated that context switching between separate interfaces increased cognitive load and reduced adoption. Radiologists were required to reconcile findings across multiple systems, creating workflow friction and liability ambiguity.
The decision was therefore architectural, not algorithmic.
By embedding AI directly into a unified diagnostic workspace — with overlay controls, explainability, audit tracking, and triage integration — the system enhances interpretation without altering established reading patterns.
This design choice was instrumental in increasing the Radiologist Trust Score from 27% to 89% within six months.
How is regulatory traceability maintained across model updates?
The development lifecycle was aligned with IEC 62304 and ISO 13485 processes from project inception.
Each model version is associated with:
- Dataset hash tracking
- Training configuration metadata
- Deployment record immutability
- CI/CD traceability gates
- Audit logs of inference behavior and clinician overrides
This structure supports a future FDA 510(k) pathway by maintaining a complete design history file and verifiable model lineage.
Is the platform dependent on a specific PACS vendor?
No.
The architecture is vendor-neutral by design and interoperates using open standards:
- DICOMweb (WADO-RS, QIDO-RS, STOW-RS)
- HL7 FHIR R4
- DICOM Structured Reports
- SAML 2.0 secure authentication
This ensures compatibility with enterprise PACS ecosystems while avoiding proprietary lock-in.
How does the system maintain performance under peak seasonal load?
The AI inference layer runs on GPU-accelerated nodes within a HIPAA-eligible cloud environment, orchestrated via Kubernetes with auto-scaling policies.
During seasonal respiratory peaks, GPU resources scale dynamically based on queue depth and workload demand. Average inference latency remains ~47 seconds per CT study, without degradation of viewer responsiveness.
This separation of rendering and inference ensures UI performance is not impacted by backend model execution.

“This initiative was not about automation — it was about capacity expansion without compromising diagnostic integrity. The platform allowed us to increase throughput while strengthening compliance posture and long-term regulatory readiness.”
Willst du ähnliches erreichen Ergebnisse? Lass uns deine Idee entwickeln!